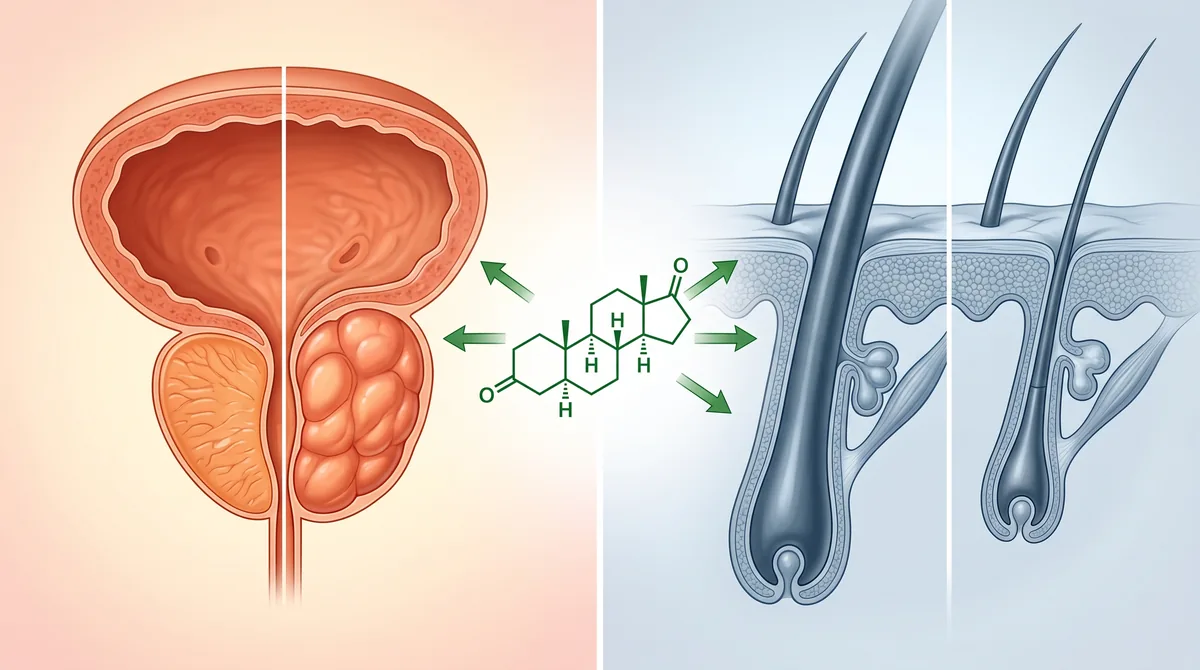
The same pill that shrinks an enlarged prostate also stops male pattern baldness. That’s not a coincidence. It’s the same mechanism.
Finasteride blocks the hormone responsible for both conditions: dihydrotestosterone, or DHT. In the prostate, DHT causes tissue overgrowth. In the scalp, it miniaturizes hair follicles. Block DHT, and you address both problems at once.
But here’s what most men don’t realize: the dose matters. A lot. The 5mg dose prescribed for benign prostatic hyperplasia (BPH) is five times stronger than the 1mg dose used for hair loss. Same drug, different applications, different risk-benefit calculations.
We’re breaking down the dual mechanism, the dosing differences, what the research shows about effectiveness for each condition, and what you need to know before starting finasteride for either reason. This is informed-consent territory. If you’re considering finasteride, this is the context you need.
The DHT Connection: Why One Drug Treats Two Conditions
Finasteride is a 5-alpha reductase inhibitor. That enzyme converts testosterone into DHT, a more potent androgen that’s three times stronger at binding to androgen receptors than testosterone itself.
In the prostate, DHT drives cell proliferation. More DHT means more tissue growth, which is why men with BPH have enlarged prostates that compress the urethra and cause urinary symptoms: weak stream, frequent urination, incomplete emptying.
In the scalp, DHT binds to receptors in genetically susceptible hair follicles and triggers miniaturization. The follicles shrink, the growth phase shortens, and eventually the follicle stops producing terminal hair. That’s androgenetic alopecia.
Finasteride reduces DHT levels by about 70% systemically. That’s enough to slow prostate growth and stop follicle miniaturization in most men. A 1999 study in The New England Journal of Medicine confirmed finasteride reduced prostate volume by 18% over four years in men with BPH.
For hair loss, a 1998 study published in the Journal of the American Academy of Dermatology showed that 1mg daily finasteride increased hair count by 15% at one year and maintained that gain at two years in men with vertex baldness.
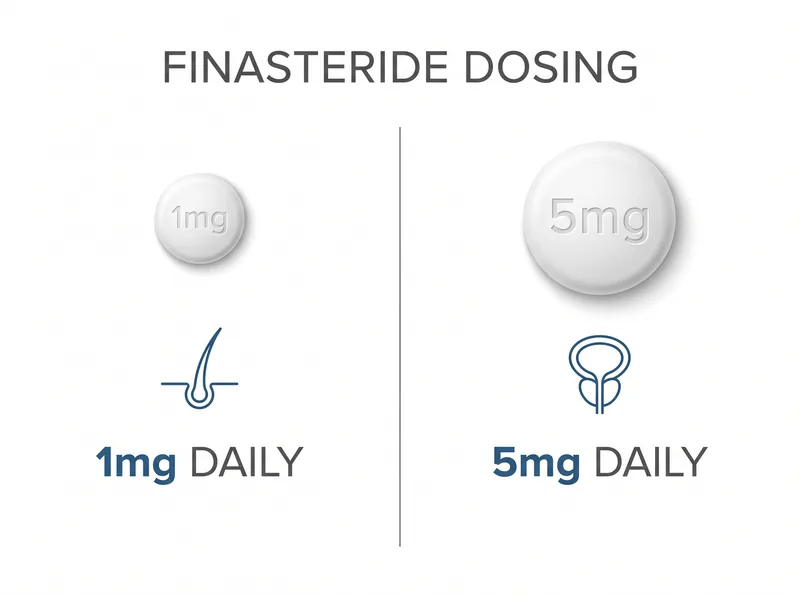 The same drug, different doses: 1mg for hair loss (Propecia), 5mg for enlarged prostate (Proscar)
The same drug, different doses: 1mg for hair loss (Propecia), 5mg for enlarged prostate (Proscar)
Dosing Differences: 1mg vs 5mg and What It Means
The FDA approved two doses of finasteride for two different conditions. Proscar (5mg) for BPH in 1992. Propecia (1mg) for male pattern hair loss in 1997.
Why the dose difference? The prostate requires more DHT suppression to achieve measurable tissue shrinkage. The 5mg dose was chosen based on clinical trials showing it reduced prostate volume and improved urinary flow rates in men with symptomatic BPH.
For hair loss, researchers found that 1mg daily was nearly as effective at reducing scalp DHT as 5mg, but with a better side effect profile. A 1999 study in the Journal of Clinical Endocrinology & Metabolism showed 1mg reduced serum DHT by 71%, while 5mg reduced it by 75%. Diminishing returns.
Some men take the 5mg dose and cut the pills into quarters to save money, since Proscar is often cheaper than Propecia. That’s a 1.25mg dose, slightly higher than the approved 1mg but functionally equivalent for hair loss purposes.
If you’re prescribed finasteride for BPH, you’re getting five times the dose used for hair. That doesn’t mean five times the benefit for hair loss. It does mean a higher likelihood of side effects, which we’ll address below.
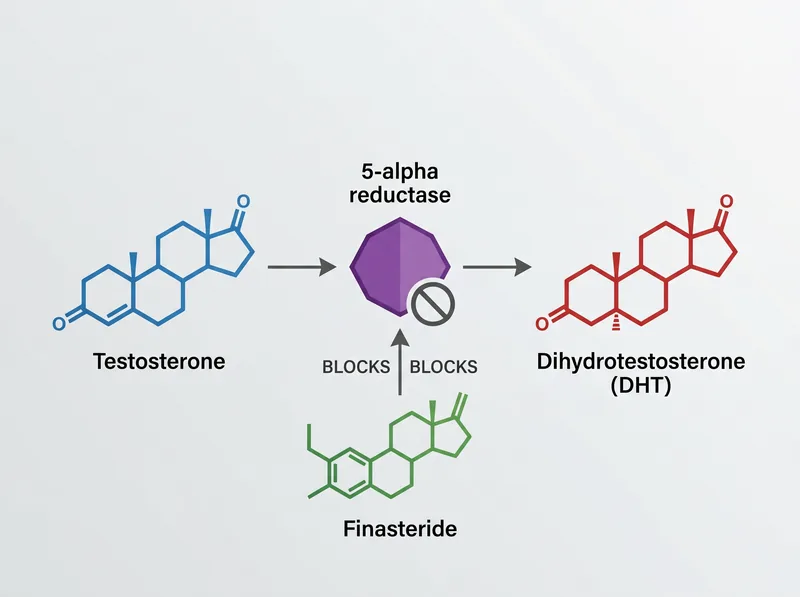 Finasteride works by blocking the enzyme that converts testosterone into DHT, the hormone responsible for both prostate enlargement and hair follicle miniaturization
Finasteride works by blocking the enzyme that converts testosterone into DHT, the hormone responsible for both prostate enlargement and hair follicle miniaturization
Effectiveness for Prostate Health: What the Research Shows
Finasteride is one of the most studied drugs for BPH. The Prostate Cancer Prevention Trial followed over 18,000 men for seven years. Finasteride reduced prostate volume, improved urinary symptoms, and reduced the risk of acute urinary retention by 57%.
It doesn’t work overnight. Prostate shrinkage takes three to six months. Symptom improvement follows a similar timeline. Men with larger prostates (over 40 grams) see more benefit than men with smaller glands.
A 2003 meta-analysis in The Cochrane Database reviewed 13 trials and concluded finasteride significantly improved urinary flow rates and reduced the need for surgery in men with moderate to severe BPH.
The alternative for BPH is alpha-blockers like tamsulosin, which relax the prostate muscle but don’t shrink the gland. Finasteride addresses the root cause: tissue overgrowth driven by DHT. Many urologists prescribe both together for faster symptom relief.
If you’re in the Gulf region and experiencing urinary symptoms, see a urologist. BPH is common after 50, and finasteride is a first-line treatment. But don’t self-prescribe the hair loss dose and expect prostate benefits. The dosing matters.
Effectiveness for Hair Loss: The Evidence Base
For male pattern baldness, finasteride is one of two FDA-approved drugs (the other is minoxidil). It works best for vertex and mid-scalp thinning. It’s less effective for frontal hairline recession.
The five-year data from the Propecia trials showed 90% of men maintained or increased their hair count. That means it stopped progression in nearly everyone, and about 65% saw visible regrowth.
Results plateau after two years. You’re not going to keep gaining hair indefinitely. The benefit is stabilization: keeping what you have, recovering some of what you lost recently, and preventing further miniaturization.
Finasteride doesn’t work for everyone. About 10% of men are non-responders, likely due to genetic variations in androgen receptor sensitivity or 5-alpha reductase enzyme activity. If you’ve been on it for a year with no change, it’s probably not going to work.
If you stop taking it, you lose the benefit within 12 months. The hair you maintained will resume miniaturizing. That’s not a rebound effect. It’s just DHT doing what it does when it’s no longer suppressed.
Side Effects: The Informed Consent Conversation
The most discussed side effects are sexual: reduced libido, erectile dysfunction, decreased ejaculate volume. In clinical trials, these occurred in 1.3% to 1.8% of men on 1mg finasteride, compared to 0.9% to 1.2% on placebo.
That’s a small absolute increase, but it’s real. Some men experience persistent symptoms even after stopping the drug. Post-finasteride syndrome (PFS) is controversial. It’s not officially recognized by regulatory agencies, but patient reports are consistent enough to warrant caution.
A 2011 study in The Journal of Sexual Medicine documented 71 men who reported persistent sexual, cognitive, and physical symptoms after discontinuing finasteride. The mechanism isn’t fully understood, but neurosteroid changeion is one hypothesis.
Other reported side effects: depression, brain fog, gynecomastia (breast tissue growth), testicular discomfort. These are less common but documented in post-marketing surveillance data.
Here’s the informed consent part: if you’re taking finasteride for hair loss, you’re trading a cosmetic benefit for a small but real risk of sexual side effects. If you’re taking it for BPH, you’re treating a medical condition that affects quality of life and can lead to complications like urinary retention or kidney damage. The risk-benefit calculation is different.
In the Gulf, where finasteride is available over the counter in some countries, men often start it without full medical counseling. That’s a problem. You should know what you’re signing up for before you take the first pill.
Dutasteride: The Stronger Alternative
Dutasteride is a newer 5-alpha reductase inhibitor that blocks both type 1 and type 2 isoforms of the enzyme. Finasteride only blocks type 2. That means dutasteride reduces DHT more completely: about 90% suppression versus 70% with finasteride.
It’s FDA-approved for BPH (as Avodart, 0.5mg daily) but not for hair loss in most countries. However, dermatologists prescribe it off-label for androgenetic alopecia, especially in men who don’t respond to finasteride.
A 2006 study in the Journal of the American Academy of Dermatology found dutasteride 0.5mg daily was more effective than finasteride 1mg for increasing hair count in men with pattern baldness.
The trade-off: a higher side effect risk. More DHT suppression means more potential for sexual and hormonal effects. Dutasteride also has a longer half-life (about five weeks versus six hours for finasteride), so it takes longer to clear your system if you stop.
For BPH, dutasteride is an option if finasteride doesn’t provide adequate symptom relief. For hair loss, it’s a second-line choice after finasteride fails. It’s not a first-line treatment unless you’re specifically looking for maximum DHT suppression.
Gulf-Specific Considerations: Availability and Monitoring
Finasteride is widely available across the Gulf, often without a prescription. That’s convenient but risky. Starting a drug that affects hormone levels without baseline blood work or medical supervision is not ideal.
Before starting finasteride for either BPH or hair loss, get a PSA (prostate-specific antigen) test. Finasteride lowers PSA levels by about 50%, which can mask prostate cancer. Your doctor needs a baseline to interpret future PSA results correctly.
In the region’s hot climate, men often attribute fatigue or low libido to heat, stress, or work schedules. But if you’re on finasteride and experiencing these symptoms, the drug could be the cause. Don’t dismiss it.
If you’re using finasteride for hair loss, consider pairing it with a chelating shampoo like Regrowth+ to address the mineral buildup from hard water that can compound scalp issues. The drug addresses DHT, but environmental factors still matter for overall hair health.
For men over 50 with both BPH symptoms and hair loss, finasteride offers dual benefits. But you need proper medical follow-up: annual PSA tests, digital rectal exams, and monitoring for side effects. Don’t treat it as a cosmetic-only intervention if you’re in the age range where prostate health becomes a clinical concern.
Who Should Consider Finasteride (And Who Shouldn’t)
You’re a candidate for finasteride if you have documented male pattern baldness (Norwood scale 3-5), you’re over 25, and you’re willing to accept the side effect risk for the benefit of hair preservation.
You’re a candidate for finasteride if you have symptomatic BPH with a prostate over 40 grams, you’re experiencing urinary flow issues, and you want to avoid surgery.
You’re not a candidate if you’re under 25. Androgenetic alopecia stabilizes later in younger men, and starting finasteride too early means decades of continuous use with cumulative side effect risk.
You’re not a candidate if you have a history of depression or sexual dysfunction. Finasteride can worsen both, and the risk-benefit doesn’t favor starting it.
You’re not a candidate if you’re trying to conceive. Finasteride reduces semen volume and may affect sperm parameters. Most men discontinue it three months before attempting conception, though the data on fertility impact is mixed.
Women of childbearing age should never handle crushed or broken finasteride tablets. The drug can cause birth defects if absorbed through the skin during pregnancy. That’s a hard safety rule.
References
- Finasteride in the treatment of men with benign prostatic hyperplasia - The New England Journal of Medicine
- Finasteride in the treatment of men with androgenetic alopecia - Journal of the American Academy of Dermatology
- Effect of finasteride on serum androgens in men with benign prostatic hyperplasia - Journal of Clinical Endocrinology & Metabolism
- Finasteride for benign prostatic hyperplasia - The Cochrane Database of Systematic Reviews
- Persistent sexual side effects of finasteride for male pattern hair loss - The Journal of Sexual Medicine