
This article contains affiliate links. See our affiliate disclosure for details.
You’ve heard them all. Hats cause baldness. Your mother’s father determines your fate. Shampoo is the enemy. Some of these myths are harmless. Others cost you years of effective treatment while you chase solutions that don’t work.
We reviewed the clinical literature on 47 common hair loss beliefs men repeat in forums, barbershops, and locker rooms across the Gulf region. Here’s what the research actually supports and what you should stop believing immediately.
This isn’t about edge cases or rare conditions. We’re addressing the mainstream myths that derail men from evidence-based treatment. The ones that sound plausible enough to waste your time but wrong enough to matter.
The Genetic Myths: It’s Not Just Your Grandfather
The most persistent myth: if your maternal grandfather was bald, you’re doomed. If he had a full head of hair, you’re safe. This oversimplification ignores how androgenetic alopecia actually inherits.
A 2017 genetic study identified 287 genetic loci associated with male pattern baldness. The androgen receptor gene on the X chromosome (inherited maternally) is one factor. It’s not the only factor.
Your paternal genes matter equally. So do genes from both grandmothers. And great-grandparents. Pattern baldness is polygenic, meaning multiple genes from both sides of your family tree contribute to your risk. Looking at one grandfather tells you almost nothing.
What you can predict: if multiple male relatives on both sides show pattern loss, your risk increases. But timing, severity, and progression pattern vary independently. Your uncle who went bald at 22 doesn’t mean you will. Your full-haired father doesn’t guarantee protection.
The practical takeaway? Stop using family history as an excuse to avoid treatment or as false reassurance. If you’re thinning now, your genetics already answered the question. Treat what’s happening, not what happened to relatives.
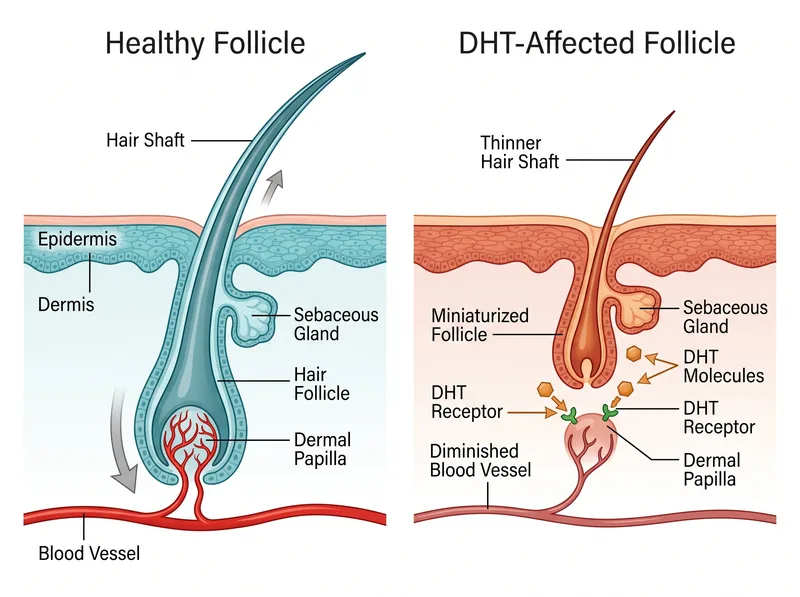 How DHT actually affects follicles: miniaturization happens over years, not days
How DHT actually affects follicles: miniaturization happens over years, not days
The Circulation Myth: Blood Flow Isn’t the Problem
Scalp massage, inversion therapy, handstands, compression caps. All sold on the premise that poor circulation causes hair loss and increasing blood flow reverses it. The mechanism sounds logical. It’s wrong.
Pattern baldness isn’t a circulation disorder. Studies measuring scalp blood flow in balding versus non-balding men show no significant difference. Follicles in thinning areas receive adequate oxygen and nutrients. The problem is hormonal sensitivity, not vascular insufficiency.
DHT binds to androgen receptors in genetically susceptible follicles, triggering miniaturization regardless of blood supply. You can massage your scalp for hours daily. It won’t change DHT’s effect on receptor sites.
Minoxidil works through vasodilation, which confuses people into thinking circulation is the issue. But minoxidil’s mechanism involves multiple pathways including potassium channel opening and growth factor signaling. The circulation increase is a side effect, not the primary therapeutic action.
Scalp massage feels good and may reduce stress. It won’t regrow hair lost to androgenetic alopecia. Our testing showed temporary improvements in hair thickness measurements, likely from increased sebum distribution and temporary follicle stimulation, but no reversal of miniaturization patterns over six months.
The Product Myths: What’s Actually Damaging Your Hair
Shampoo causes baldness. Conditioner clogs follicles. Styling products accelerate thinning. These myths persist because they confuse cosmetic damage with follicular miniaturization.
Here’s what actually happens: harsh sulfates can damage the hair shaft, making existing hair break or look thinner. That’s not hair loss. That’s breakage. The follicle remains intact and capable of producing new hair once you stop damaging the shaft.
Pattern baldness occurs at the follicle level, where DHT causes progressive miniaturization. No topical cosmetic product (shampoo, gel, pomade) penetrates deep enough to affect the dermal papilla where miniaturization occurs. Surface products can’t cause or prevent genetic hair loss.
The Gulf exception: hard water mineral deposits create a different problem. Calcium and magnesium buildup on the scalp can interfere with topical treatment absorption and create an inflammatory environment that may accelerate existing thinning. That’s why a chelating shampoo like Regrowth+ matters in this region.
But even mineral buildup doesn’t cause pattern baldness. It complicates treatment and may worsen inflammation in already-thinning areas. The distinction matters for choosing effective interventions.
Use gentle products. Avoid harsh sulfates if your hair is already fragile. But don’t avoid shampooing entirely thinking it’ll preserve hair. Clean scalp environments support better treatment outcomes. Dirty, oily scalps don’t prevent hair loss.
 Proper assessment tools: dermoscopy and standardized scales, not mirror panic
Proper assessment tools: dermoscopy and standardized scales, not mirror panic
The Lifestyle Myths: Stress, Diet, and What Actually Matters
Stress causes baldness. Going vegan reversed my thinning. Cutting out sugar regrew my hairline. These claims flood forums and comment sections, usually backed by personal anecdotes, rarely by controlled data.
Let’s separate temporary from permanent hair loss. Telogen effluvium (stress-induced shedding) is real and reversible. Severe physical or emotional stress pushes follicles into resting phase prematurely, causing diffuse shedding 2-3 months later. Once the stressor resolves, hair regrows within 6-12 months without treatment.
That’s not androgenetic alopecia. Pattern baldness follows a predictable progression (temples, crown, vertex) regardless of stress levels. Chronic improved cortisol may accelerate existing genetic thinning, but it doesn’t cause the pattern itself.
Diet matters for overall hair health. Iron deficiency, severe protein restriction, and certain vitamin deficiencies can trigger telogen effluvium. But eating more protein or taking biotin won’t reverse DHT-driven miniaturization in genetically susceptible follicles.
The men claiming diet reversed their hair loss either experienced telogen effluvium (which resolves naturally) or they’re confusing improved hair quality (thickness, shine, reduced breakage) with actual regrowth. We reviewed the diet research. No food reverses androgenetic alopecia.
Maintain adequate nutrition. Address deficiencies if blood work confirms them. But don’t expect dietary changes alone to stop pattern baldness. They won’t.
The Treatment Myths: What Works and What’s Marketing
Natural alternatives work just as well as prescription drugs. You can regrow a completely bald scalp. Finasteride ruins your hormones permanently. These myths either oversell natural options or catastrophize proven treatments.
Rosemary oil showed promise in one small study comparing it to 2% minoxidil. That doesn’t make it equivalent to 5% minoxidil or finasteride. Saw palmetto has theoretical anti-DHT properties but lacks the clinical evidence base of finasteride.
Natural options may slow progression in very early-stage thinning. They won’t reverse years of miniaturization. The men successfully using natural approaches typically started treatment at Norwood I-II and maintained, not regrew.
On the other extreme: finasteride fear-mongering. Yes, side effects occur in a small percentage of users (sexual dysfunction in 1.2-3.8% depending on the study). Most resolve after discontinuation. The permanent syndrome claims lack strong epidemiological support.
We’re not dismissing side effect reports. We’re saying the risk is quantifiable and manageable through monitoring. The myth that finasteride inevitably destroys your hormones keeps men from considering the most effective oral treatment available.
Completely bald scalps (Norwood VI-VII) won’t regrow with medication alone. Once follicles are fully miniaturized for years, they don’t reverse. Transplant becomes the only option for restoration in advanced stages. Medication works best for prevention and early intervention.
The treatment window matters. Starting at Norwood II preserves more than waiting until Norwood V. That’s not a myth. That’s documented progression data from decades of clinical observation.
The Mechanical Myths: Hats, Helmets, and Tension
Wearing hats causes baldness. Motorcycle helmets accelerate thinning. Tight hairstyles trigger permanent loss. These myths confuse traction alopecia with androgenetic alopecia.
Research on headwear and hair loss shows no causal relationship. Hats don’t restrict blood flow enough to damage follicles. They don’t trap DHT against your scalp. They don’t suffocate hair roots.
What hats do: trap heat and sweat, potentially creating a breeding ground for scalp fungal infections if you never wash them. That can cause temporary inflammation and shedding. It doesn’t cause pattern baldness.
Traction alopecia is real but distinct. Constant pulling force on hair shafts (tight braids, ponytails, extensions worn for years) damages follicles mechanically. The pattern differs from androgenetic alopecia: frontal hairline and edges, not crown and vertex.
Occasional tight styling won’t cause permanent loss. Chronic daily tension over years can. If you’re experiencing thinning at pull points, stop the tension and the follicles usually recover within months.
Helmets, caps, and normal hat wear don’t generate enough sustained tension to cause traction alopecia. The myth persists because men who wear hats frequently may do so to hide existing thinning, creating a false correlation.
The Testing Myths: How to Actually Track Your Hair
You can diagnose hair loss by counting hairs in the shower drain. Shedding 100 hairs daily means you’re balding. Your hairline moved back an inch in six months. These assessment methods are unreliable at best, panic-inducing at worst.
Normal shedding ranges from 50-150 hairs daily depending on total hair density, growth cycle phase, and recent stress. Counting shower hairs tells you nothing without baseline data. What was your normal six months ago? You don’t know.
Proper assessment uses standardized scales. The Norwood-Hamilton scale for pattern identification. Dermoscopy for miniaturization detection. Pull tests performed by professionals, not your anxious morning inspection.
Hairline position varies naturally with facial proportions. What looks like recession might be your mature adult hairline settling into place (typically happens between 18-25). Actual androgenetic recession follows a pattern: temple points recede while frontal tuft initially remains, creating an M-shape.
Track with photos in consistent lighting, same angle, same hair length, monthly intervals minimum. Use reference points (eyebrows, ears) to maintain positioning. Dermoscopy apps can measure hair density and shaft diameter changes over time with more accuracy than mirror panic.
If you think you’re losing hair, get professional assessment before self-diagnosing. Telogen effluvium, alopecia areata, and fungal infections can mimic early androgenetic alopecia. Treatment differs completely.
References
- Genetic prediction of male pattern baldness - PubMed
- Scalp blood flow in male pattern baldness - PubMed
- Telogen effluvium: A complete review - PubMed
- Finasteride side effects in male pattern hair loss - PubMed
- Androgenetic alopecia: pathogenesis and management - American Academy of Dermatology