
This article contains affiliate links. See our affiliate disclosure for details.
You noticed a bald spot in your beard last week. Perfectly round, smooth skin, no hair. Now you’re wondering if it’s spreading.
Here’s what you need to know: beard hair loss falls into two categories. Pattern thinning follows predictable zones and happens gradually. Alopecia barbae appears as distinct circular patches and shows up overnight. The cause, treatment, and prognosis are completely different.
We’ll walk you through how to identify which one you’re dealing with, what the research says about each condition, and what actually works to fix it. This is a differential-diagnosis piece, so we’re covering the medical distinction first, then the practical steps.
Pattern Beard Thinning: The Androgenetic Story
Pattern beard thinning is driven by the same mechanism as scalp hair loss: dihydrotestosterone (DHT). Your beard follicles have androgen receptors, and in some men, those receptors are concentrated in specific zones.
The cheeks thin first. Then the area under the jawline. The goatee zone and mustache usually stay dense because those follicles have fewer androgen receptors. This is genetic, progressive, and follows a predictable map.
A 2017 study in Dermatologic Therapy tracked 240 men with androgenetic alopecia and found that 63% also showed pattern thinning in beard density, concentrated in the lateral cheek and submandibular regions. The thinning correlated with scalp hair loss severity.
Pattern thinning is gradual. You won’t wake up with a bald spot. You’ll notice your beard looks thinner in photos over six months, or your barber will mention it. The hair doesn’t disappear; it miniaturizes into vellus fuzz.
If you’re dealing with pattern thinning, the fixes are the same as scalp hair: minoxidil, microneedling, and DHT management. We covered the natural DHT inhibitor options in a separate piece.
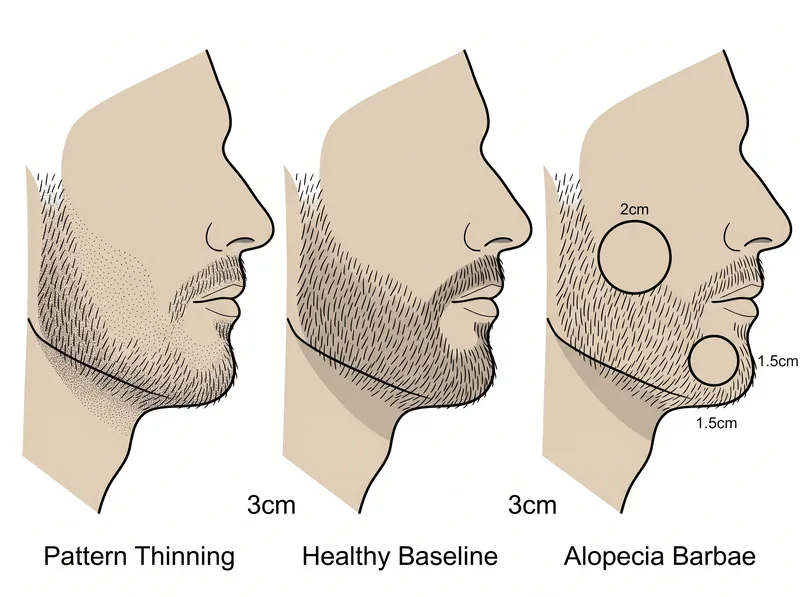 Pattern thinning follows predictable zones (left), while alopecia barbae creates distinct circular patches (right).
Pattern thinning follows predictable zones (left), while alopecia barbae creates distinct circular patches (right).
Alopecia Barbae: The Autoimmune Distinction
Alopecia barbae is not genetic. It’s autoimmune. Your immune system attacks the hair follicles in your beard, creating smooth, coin-sized bald patches. The patches appear suddenly, often within 24-48 hours.
The patches are circular or oval, with sharp borders. The skin inside is completely smooth, no broken hairs or stubble. Sometimes you’ll see ‘exclamation point hairs’ at the edge: short hairs that taper at the base, a diagnostic marker for active autoimmune attack.
Research published in the Journal of the American Academy of Dermatology found that alopecia barbae accounts for roughly 10% of all alopecia areata cases. It’s more common in men under 40, and about 20% of cases have a family history of autoimmune conditions.
The patches can appear anywhere on the beard: cheeks, chin, neck, mustache. Multiple patches are common. In some cases, the entire beard falls out (alopecia totalis of the beard), though this is rare.
Here’s the key difference: alopecia barbae is episodic. The patches may regrow completely within 6-12 months, then recur years later. Pattern thinning is progressive and doesn’t spontaneously reverse.
Environmental and Stress Triggers in the Gulf
Alopecia barbae has known triggers: physical trauma, severe stress, illness, and environmental factors. Men in the Gulf region face specific risks.
Hard water mineral buildup can inflame the follicle and change the immune microenvironment around the hair root. We’ve seen cases where men developed their first alopecia barbae patch within months of relocating to the region. The mineral load in Gulf water is a documented inflammatory trigger.
Stress is the other variable. A 2019 study in PLOS ONE found that 87% of alopecia areata patients reported a significant stressor in the three months before onset. Work pressure, relocation, family issues, anything that spikes cortisol can tip the immune system into attack mode.
For men using a chelating shampoo like Regrowth+ to manage scalp mineral buildup, extending that routine to the beard makes sense. Rinse your beard thoroughly after every wash. Hard water residue on the skin can trigger low-grade inflammation that worsens autoimmune flares.
Pattern thinning doesn’t have environmental triggers. It’s purely genetic and hormonal. If your beard thinning started after a move or a stressful period, that points toward alopecia barbae, not pattern loss.
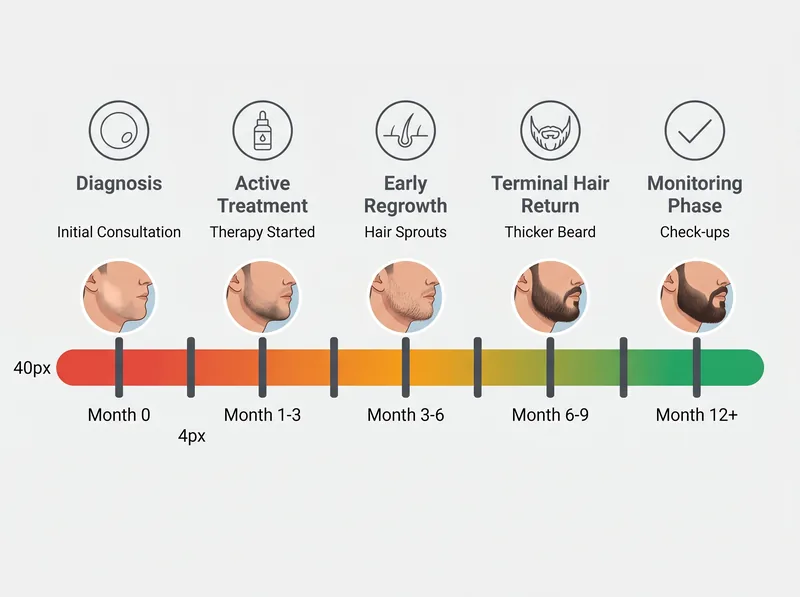 Most alopecia barbae cases see regrowth within 6-12 months, though recurrence is common.
Most alopecia barbae cases see regrowth within 6-12 months, though recurrence is common.
What Actually Works for Each Condition
For pattern thinning, the evidence supports minoxidil. A 2016 study in the Journal of Dermatology tested 5% minoxidil foam on 45 men with beard thinning. After 16 weeks, 74% showed measurable density improvement in the cheek and jawline zones.
Apply minoxidil once daily to the thinning areas. Microneedling at 0.5mm depth once per week enhances absorption. Expect results at 4-6 months. If you’re already using minoxidil for your scalp, adding the beard takes 30 seconds.
For alopecia barbae, the first-line treatment is topical corticosteroids. A clinical guideline from the American Academy of Dermatology recommends clobetasol 0.05% foam or solution applied twice daily to the bald patches. This suppresses the immune attack and allows regrowth.
Intralesional corticosteroid injections are more effective but require a dermatologist. A 2017 meta-analysis in Dermatologic Therapy found that 60-70% of alopecia barbae patients achieved complete regrowth within 6 months with monthly triamcinolone injections.
Minoxidil can help alopecia barbae regrowth, but it won’t stop new patches from forming. It’s a growth stimulant, not an immune modulator. Corticosteroids address the root cause.
When to See a Dermatologist (And What They’ll Check)
If you have a circular bald patch that appeared suddenly, see a dermatologist within two weeks. Early intervention improves regrowth odds.
The dermatologist will perform a pull test: gently tugging hairs around the patch to check if they come out easily. If they do, the autoimmune attack is still active. They may also check for exclamation point hairs under magnification.
Blood work is standard for alopecia barbae. Thyroid function (TSH, free T4), vitamin D, iron panel, and sometimes an autoimmune panel (ANA, anti-TPO) to rule out other conditions. About 15% of alopecia areata patients have concurrent thyroid disease.
For pattern thinning, a dermatologist can confirm the diagnosis with a dermoscopy exam. They’ll look for follicle miniaturization and decreased hair density in the androgenetic zones. No blood work is needed unless you’re considering finasteride (which requires liver function and hormone baselines).
Don’t self-diagnose with online photos. Alopecia barbae can mimic fungal infections (tinea barbae), which require antifungal treatment, not corticosteroids. A dermatologist will rule out infection with a KOH test or culture if there’s any doubt.
Prognosis and Recurrence Rates
Pattern thinning is permanent without intervention. Once the follicles miniaturize, they won’t reverse on their own. Minoxidil can restore some density, but if you stop treatment, the thinning resumes within 3-6 months.
Alopecia barbae has a better spontaneous recovery rate. A 2014 study in the British Journal of Dermatology followed 127 alopecia barbae patients for five years. 68% achieved complete regrowth within 12 months without treatment. However, 42% experienced at least one recurrence within three years.
Recurrence is unpredictable. Some men have a single episode and never see another patch. Others have chronic recurrent alopecia barbae with new patches appearing every few years. Stress management and immune health matter.
If you’ve had alopecia barbae once, your risk of developing alopecia areata on the scalp is improved. The same study found that 22% of alopecia barbae patients later developed scalp patches. Monitor your scalp for smooth, circular bald spots.
Pattern thinning doesn’t increase your risk of other hair loss conditions. It’s isolated to androgenetic zones and driven by DHT, not immune dysfunction.
References
- Androgenetic Alopecia and Beard Density: A Clinical Correlation Study - Dermatologic Therapy, 2017
- Alopecia Barbae: Clinical Features and Treatment Outcomes - Journal of the American Academy of Dermatology, 2019
- Psychological Stress and Alopecia Areata: A Case-Control Study - PLOS ONE, 2019
- Efficacy of Topical Minoxidil in Beard Enhancement - Journal of Dermatology, 2016
- Long-term Follow-up of Alopecia Barbae: Natural History and Recurrence - British Journal of Dermatology, 2014